
What is a salivary stone?

Parotid gland

Sub-mandibular gland
Salivary stones form in the salivary glands: mainly in the sub-mandibular gland (80%), less frequently in the parotid glands (20%), and extremely rarely in the sublingual glands and minor salivary glands of the mouth. The salivary glands normally secrete calcium but, under conditions that favour salivary stasis (salivary duct anomalies, retrograde oral infections, dehydration), the aggregation of calcium crystals leads to the formation of a macroscopic stone. The presence of the stone impedes the normal outflow of saliva (particularly when it is stimulated during a meal) and causes “salivary colic”: i.e. a painful swelling in the sub-mandibular (lower jaw) or parotid region (near the ear). Even the simple “mouth watering” stimulated by some pleasant-tasting foods can give rise to salivary colic and cause considerable discomfort during a family or working lunch or dinner. The next step is acute purulent sialadenitis (an infection of the gland and ductal system) that requires antibiotic treatment.
What causes “salivary colic”?
Stones are the main cause (63-79%), but the salivary glands become obstructed for other reasons, such as:
- Salivary duct anomalies (stenosis or narrowing, acute angulations, “kinking”, ductal invaginations);
- Dense mucous plugs;
- Polyps and granulated tissue due to autoimmune diseases such as Sjögren’s syndrome;
- External compression (hypertrophy of nearby muscles such as the masseter muscle in bruxism or the myloyoid muscle, inflamed lymph nodes);
- Foreign bodies (vegetable fibres, pieces of toothpick, food remnants).
How is it diagnosed?
Diagnosis begins with an otorhinolaryngoiatric (ENT) examination that makes it possible to detect a stone visually in the mouth or by means of palpation. If no stone is found during this examination, the further diagnostic investigations include:
- Ultrasonography and colour Doppler ultrasonography of the salivary glands, which makes it possible to identify most salivary stones, including those that are not radiopaque;
- Mouth radiography (like that used by dentists) and lateral radiography of the lower jaw in order to detect submandibular stones;
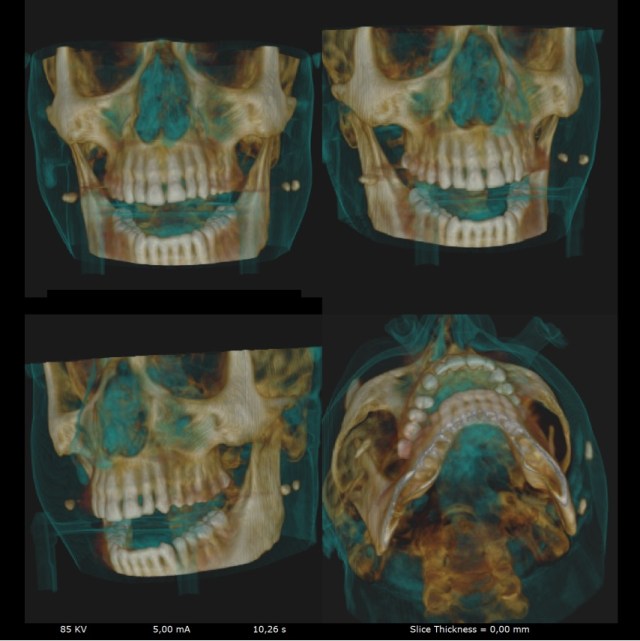
- A cone beam 3D computed tomography (TC) scan for parotid and submandibular stones that cannot be seem ultrasonographically;
- Sialo-MR (magnetic resonance) imaging when salivary duct dilation or stenosis (narrowing) is suspected in the absence of salivary stones;
- Salivary gland video-endoscopy if the results of the radiological examinations are not sufficient for diagnosis.
What is sialendoscopy?
Salivary gland video-endoscopy is a new method that makes it possible to explore the salivary duct system when looking for the cause of an obstruction (stones, duct anomalies, etc.). It is typically performed using local anesthesia or a nerve block (like that used by dentists). The endoscopes are very thin in order to allow entry into the small ducts (the dilated diameter of which is no more than 2 mm after irrigation with saline solution): a diagnostic endoscope has a diameter of 0.8 mm, and those with operating channel have a diameter of 1.1 and 1.6 mm.
How are salivary stones removed?
Salivary stones can be endoscopically removed using the following instruments:
- Variously sized baskets;
- Micro-tweezers to break up stones and remove the fragments;
- A laser or pneumatic fibre inserted in the operating channel of an endoscope.
What happens in the case of a salivary duct stenosis?
If the findings of the radiological examinations indicate a stenosis (narrowing) in a salivary duct, it is possible to dilate the stenosis video-endoscopically and then insert a stent (a small tube) to keep it open.
Is it possible to break up stones using shock waves?
Extracorporeal shock wave lithotripsy (fragmentation) is one of the most widely used means of breaking up salivary stones. Originally used to treat kidney stones, it can be used for:
- all parotid stones bigger than 2.5 mm;
- all sub-mandibular stones of between 2.5 and 7 mm.
No anesthesia is necessary, and it takes an average of five 30-minute lithotripsy sessions to break up the stones into sufficiently small fragments.
When can a laser or a pneumatic fiber be used to pulverise a stone?
One of the limitations of interventional sialo-endoscopy is that it is difficult to remove stones that are bigger than 4 mm using the traditional operative instruments (a drill, baskets and micro-tweezers); consequently, the first step in the removal of larger stones is to break them up into small pieces that that can be naturally flushed out during normal salvation or removed operatively. This can be done using extracorporeal shock wave equipment or endoscopically guided intracorporeal instruments such as a laser or pneumatic devices. Over the last few years, lasers have come more widely used in urology and otorhinolaryngology. The most widely used are holmium:YAG lasers, and there is enough data to support their safety and effectiveness in salivary gland treatment. However, one of the side effects of this technique is the possibility of inducing a ductal stenosis. A new lithotripsy approach is represented by pneumatic lithotripsy through the working channel of a 1.3 mm salivary endoscopic device. The current indications for sialo-endoscope assisted intracorporeal laser or pneumatic lithotripsy are stones that fail to respond to extracorporeal shock wave lithotripsy and stones of between 4 and 7 mm in diameter).
What technique is preferable in the case of very large stones?
- Very large parotid stones of about 1 cm are initially treated by means of extracorporeal lithotripsy and, if this fails, sialendoscopy-assisted surgical removal under general anesthesia can be proposed;
- In the case of very large sub-mandibular stones, the preferred technique is sialendoscopy-assisted surgical removal through their mouth under general anesthesia.
Is it possible to preserve submandibular salivary gland in the case of a deep and big stone?
Since 2003 it has been available sialendoscopy-assisted transoral removal of stones bigger than 5 mm located in the deep portion of Wharton’s duct or in the hilum and parenchyma of the gland with complete preservation of the duct system and salivary function. Fundamental condition to remove the stone is that it needs to be palpated by the hands into the oral floor; the patient has to undergo ultrasonography to identifiy the exact location and size of the stone. In the case of unadequate ultrasonographic detection a cone beam CT of the oral floor is wellcome to plan surgery. The surgical procedure is preferably done under general anaesthesia and is actually the most widely used procedure to cure salivary stones, even more frequent than sialendoscopy and lithotripsy. Thanks to all these techniques it is nowadays possible to save 95% of involved salivary glands. The biggest stone removed by using the proposed technique measured 38 mm.
Is it possible to preserve the parotid gland with a deep and big stone unresolved by sialendoscopy and lithotripsy techniques?
Since 2010 it has been available sialendoscopy-assisted transfacial removal of big and deep stones located in the main parotid duct and parenchyma (through a minimal cutaneous incision near and around the ear). Fundamental condition to remove the stone is that it needs to be palpated under the skin and it needs to be clearly identified in size and location by ultrasonography (bigger than 5 mm). If the stone is not clearly visible it is possible to perform a low radiation cone beam CT. The skin incision is done on a cutaneous fold near and around the external ear to minimize postoperative scar. It is possible to plan an ultrasonographic guidance during surgery in the case of deep and unpalpable stones. The procedure is done under general anaesthesia.
Figure showing the minimal cutaneous incision done to remove parotid stone by sialendoscopy-assisted transfacial technique.

When is it necessary to have a salivary gland removed?
The use of the conservative and mini-invasive techniques described above now makes it possible to preserve the glans in the vast majority (about 95%) of cases, thus avoiding the risks associated with the operation itself: aesthetic skin damage, neurological injury (the facial, lingual and hypoglossal nerves) and functional impairment.
Are there any non-surgical treatments?
The non-surgical treatments include botulinic therapy: i.e. injecting botulin toxin into the salivary gland in order to block the secretion of saliva and favour its functional silencing (rest). It is mainly used in the case of unexplained recurrent parotitis (inflammation), but it is also used in the case of salivary fistulae and sialoceles (localised subcutaneous saliva-filled cavities near the salivary glands caused by traumas or infections). Finally, it is used to treat Frey’s syndrome and sialorrhea (increased salivation) due to neurological causes (e.g. infantile cerebral paralysis, Parkinson’s disease).
What is Frey’s syndrome?
It is characterised by profuse sweating in the parotid region. It is usually due to parotidectomy (the removal of the parotid gland) and is often associated with a reddening of the skin. It is diagnosed by means of Minor’s starch-iodine test (the photograph shows the area of sweating).

It is treated by injecting botulin toxin under the skin in the affected area. The action of toxin lasts for an average of four months and so, in some cases, it is necessary to repeat the treatment.
What is recurrent pediatric parotitis?
It is an inflammatory condition that is characterised by recurrent and often painful swelling of one or both of the parotid glands, which occurs at least before the age of puberty. It is the second most frequent pediatric salivary gland disorder after epidemic parotitis (mumps). Its origin is still unclear, although it seems to be favoured by the activation of mucosa-associated lymphatic tissue (MALT) in the salivary glands. It leads to the release of inflammatory mediators, and the inflammation around the salivary ducts reduces their lumens and obstructs normal salivary flow. It can be easily diagnosed by means of of salivary gland ultrasonography and MR sialography (nuclear magnetic resonance) imaging.

It can be medically treated with steroidal or non-steroidal anti-inflammatory agents, a new therapeutic proposal is parotid sialendoscopy, which can be used to dilate the narrowed salivary ducts gradually by means of saline solution or the use of baskets, a procedure that is concluded by flushing the gland with anti-inflammatory steroids.
What is autoimmune recurrent sialadenitis?
It is an inflammatory condition that is characterised by recurrent and often painful swelling of one or multiple salivary glands, mainly parotid glands, which occurs during meals or independently. It is generally associated with primary or secondary Sjogren’s syndrome. Diagnosis is based on clinical history, dynamic power Doppler ultrasonography, autoimmunity blood examinations and labial minor salivary gland biopsy. Medical therapy is based on steroid and antibiotic therapy with known untoward effects and resistance. Sialendoscopy exploration and dilation with outpatient oral duct steroid irrigations is able to reduce the number of acute swelling of the glands and to improve the quality of life of patients.
